Dr. Ara Nazarian suggests a treatment solution that results in more control and fewer appointments
Having the ability to take a patient from point A-Z in a fewer amount of appointments within your practice allows you to position yourself as a provider who can fulfill your patient’s surgical and restorative needs. With the proper training, a dental provider may provide extraction, grafting, and implant placement within one appointment at one location. Not only does this allow you to reduce the amount of visits for the patient, but this type of service also helps stay within the patient’s budget. Most importantly, this enables the dental provider full control of the surgical and prosthetic outcome. Depending on the patient’s desires, the clinical conditions of the oral environment present, and the skills of the provider, a dentist may choose to extract teeth, level bone, and graft with simultaneous dental implant placement.
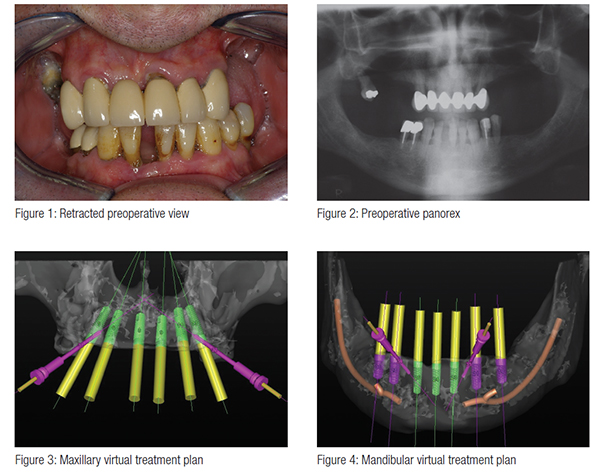
A patient in his mid-60s presented to the office with discomfort due to multiple rampant caries and generalized advanced periodontal disease (Figures 1 and 2). Having already visited multiple providers for a consultation, he was very frustrated with the treatment options offered due to varying treatment plans that were segmented by different disciplines. Since many of these options did not complement the other, the patient decided to come to us for full treatment (A-Z) after being referred to us by one of our patients who had already undergone a Total Dental Solutions Reconstruction™.
Before the surgical appointment, a CBCT scan was taken to accurately treatment plan this case to make certain that no complications would arise from doing all the procedures (extract, graft, and implant placement) in the Total Dental Solutions Reconstruction protocol. SimPlant® software (Materialise Dental, Glen Burnie, Maryland) was used through 3D Diagnostix virtual assistance to precisely plan the placement of six Engage™ (OCO Biomedical) dental implants in the maxillary arch, as well as seven Engage dental implants in the mandibular arch, using CT-based surgical pilot guides (Figure 3 and 4). The final treatment plan desired was fixed bridges on implants in the upper and lower arches.
Engage dental implants were selected (Figure 5) because I have personally experienced their high implant stability at placement, which is a critical success factor during the early healing process of osseointegration with these types of cases. With the combination of their patented Bull Nose Auger™ tip and Mini Cortic-O Thread™, the Engage (OCO Biomedical) implant system offers practitioners a bone level implant with high initial stability for selective loading options. In fact, the Engage (OCO Biomedical) implant body creates a tapping pattern when threaded for an enhanced mechanical lock in the bone. Other dental implant systems with aggressive threading may include but are not limited to NobelActive (Nobel Biocare®), Seven (MIS), ETIII (Hiossen), I5 (AB Dental USA), and AnyRidge® (Megagen).
In order to be effective and more proficient during these Total Dental Solutions Reconstruction procedures, I will utilize IV sedation. Not only does it make the appointment easier for me, but also patients prefer to get everything done in one visit. Since they are sedated, a mouth prop is needed to keep their mouth open. Because of this, I will routinely extract teeth in quadrants starting from the upper left to the upper right and then down to the lower right and lower left. This allows great time savings as it is easier to keep the patient’s mouth open and be able to proceed around the arches safely.
Once the teeth are extracted, I will reflect the tissue in order to get the bone level surgical guides seated and fixed with their respective retention pins. Using these pilot surgical guides provided by 3D Diagnostix, the sites for the implants were begun with a 1.95 mm pilot drill utilizing the Mont Blanc surgical handpiece and Aseptico surgical motor (AEU 7000) at a speed of 1200 rpm with copious amounts of sterile saline (Figures 6 and 7).
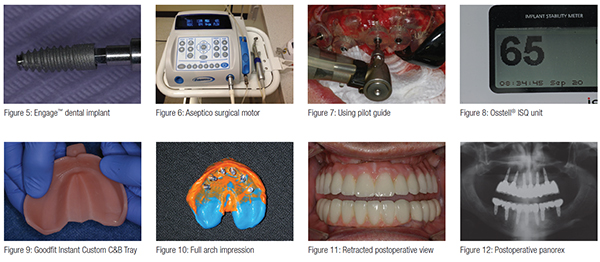
Paralleling pins were placed in the sites of the osteotomies to confirm the accuracy of the surgical guide, and X-rays were taken to check the angulations of the pins within the maxilla and the mandible. Once the osteotomies were complete, an implant finger driver was used to place the Engage dental implants until increased torque was necessary. The ratchet wrench was then connected to the adapter, and the implants torqued to final depths reaching a torque level of about 50-60 Ncm. Adequate implant fixation was further verified using an Osstell® implant stability quotient (ISQ) implant stability meter (Osstell), which uses resonance frequency analysis as a method of measurement (Figure 8). Several studies have been conducted based on resonance frequency analysis (RFA) measurements and the ISQ scale. They provide valid indications that the acceptable stability range lies above 55 ISQ.
Extended healing caps were hand-tightened to the implants. A postoperative radiograph was made of the implants and the healing caps to ensure complete seating. The immediate dentures were soft relined with a silicone-based soft denture relining material Ufi Gel SC (VOCO America). Some of the advantages I have personally experienced with this material are that it is biocompatible, tasteless, and odorless.
By using the extended healing caps with the soft reline, the immediate dentures were much more retentive. The soft tissue and implants were evaluated clinically after 1 week. The patient stated he had very little postoperative discomfort or swelling.
Within 10 days, the patient returned to the dental office. The soft tissue around the extended healing caps healed very nicely with a healthy pink color. Using impression posts, full arch impressions were taken using Instant Custom C&B Trays (Goodfit). These custom trays can be adapted and fitted in minutes, eliminating the need for models, light cure materials, monomers, and extra laboratory time in custom impression tray fabrication because they are made of a material, polymethyl methacrylate (PMMA), that becomes adjustable when heated (Figure 9) and maintains its shape while cooling. Once molded for the patient, full arch impressions were taken using a polyvinylsiloxane impression material (Take 1® Advanced, Kerr®) (Figure 10). Bite relations, as well as instructions for size, shape, and color for full arch provisionals, were forwarded to the dental laboratory. With only a 5-day turnaround, the custom abutments and provisionals were forwarded to the dental office and inserted. The patient was very pleased with the esthetics and function of these provisional restorations. He was instructed about their care and use in eating, speaking, and biting.
Approximately 4 months after the initial placement of the dental implants, the patient returned for the definitive porcelain fused to metal restoration impressions. The provisional restorations were removed using the Pneumatic Crown and Bridge Remover (DentCorp). Any temporary cement was removed and the abutments inspected. If there was any settling or recession of the gingival tissue, the abutments were modified using a carbide bur with copious amounts of water so as not to overheat the abutments. This way, the margins could be brought right at or slightly below the free gingival marginal area. A full arch impression was taken in a similar fashion for the abutments and the provisionals. In addition, the relations between maxillary and mandibular arches were captured. Within 3 weeks, the porcelain fused to metal restorations were inserted and a panorex taken (Figures 11 and 12).
More and more patients are presenting to dental practices requiring this type of reconstruction. By providing multiple services in a shorter number of visits with the use of CBCT and other technologies, you, the dental provider, will find more patients who will accept treatment. In doing so, you are not only helping your patients get to proper form and function, but also helping them achieve a Total Dental Solutions Reconstruction in a fewer amount of appointments.
 Ara Nazarian, DDS, DICOI, maintains a private practice in Troy, Michigan, with an emphasis on comprehensive and restorative care. He is a Diplomate in the International Congress of Oral Implantologists (ICOI). His articles have been published in many of today’s popular dental publications. Dr. Nazarian is the director of the Reconstructive Dentistry Institute. He has conducted lectures and hands-on workshops on esthetic materials and dental implants throughout the United States, Europe, New Zealand, and Australia. Dr. Nazarian is also the creator of the DemoDent patient education model system. He can be reached at (248) 457-0500 or at the website www.aranazariandds.com
Ara Nazarian, DDS, DICOI, maintains a private practice in Troy, Michigan, with an emphasis on comprehensive and restorative care. He is a Diplomate in the International Congress of Oral Implantologists (ICOI). His articles have been published in many of today’s popular dental publications. Dr. Nazarian is the director of the Reconstructive Dentistry Institute. He has conducted lectures and hands-on workshops on esthetic materials and dental implants throughout the United States, Europe, New Zealand, and Australia. Dr. Nazarian is also the creator of the DemoDent patient education model system. He can be reached at (248) 457-0500 or at the website www.aranazariandds.com
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
