Dr. Ara Nazarian illustrates a comprehensive implant treatment plan
When patients present to your dental practice with non-restorable teeth requiring full mouth extractions, the biggest concern is whether or not implants can be placed at the same surgical visit and, if so, will patients be able to walk out with fixed teeth? Having an implant within your practice that allows you to load or progressively load, so that these patients’ demands are met, allows you to position your practice to a whole new level. Of course, certain parameters must be met in order to facilitate this type of treatment.
[userloggedin]
This includes, but is not limited to, the quality and quantity of bone, the presence of infection, the patient’s health, and the skills of the dental provider. Additionally, the selection of the most appropriate materials for the most ideal situation must be met.
 A patient presented to my practice for a consultation wanting to restore his smile (Figure 1). He complained of generalized discomfort in his entire dentition probably due to the caries and periodontal disease that was already present (Figures 2-3). Having already visited multiple providers for an evaluation, he was very frustrated with conflicting treatment options offered. Either the suggested treatment would require multiple surgical and restorative visits that would extend for a very long time, or dental treatment would require a team approach where little coordination by dentist and specialist was communicated to the patient. Since many of these options did not appeal to him, the patient decided to have me provide comprehensive treatment that would include extractions, bone leveling, grafting, dental implant placement, immediate provisionalization, and prosthetic rehabilitation within my own practice.
A patient presented to my practice for a consultation wanting to restore his smile (Figure 1). He complained of generalized discomfort in his entire dentition probably due to the caries and periodontal disease that was already present (Figures 2-3). Having already visited multiple providers for an evaluation, he was very frustrated with conflicting treatment options offered. Either the suggested treatment would require multiple surgical and restorative visits that would extend for a very long time, or dental treatment would require a team approach where little coordination by dentist and specialist was communicated to the patient. Since many of these options did not appeal to him, the patient decided to have me provide comprehensive treatment that would include extractions, bone leveling, grafting, dental implant placement, immediate provisionalization, and prosthetic rehabilitation within my own practice.
When presenting cases like this to my patients, I will always use the Dine Digital Solution camera (Lester A. Dine, Inc.). This camera not only is small, light, and waterproof, but also is very effective and clear in taking close-up photos as well as full-face shots. Additionally, I will always offer my patients a third-party payment option like the Lending Club (San Francisco, California) for their treatment. Lending Club Patient Solutions provides patients great funding flexibility with very low rates and high approvals. Most of all, the support from their staff has been very professional.
Planning
A CBCT scan using the CS 8100 3D (Carestream Dental) was taken to accurately treatment plan this case to make certain that no complications would arise from doing all the procedures (extract, graft, and implant placement) within one visit. Since his entire dentition had caries as well as periodontal disease, his treatment would require extracting all his remaining teeth.
To further develop a treatment plan, diagnostic models were forwarded to the dental lab and mounted on the articulator for further analysis in order to meet the patient’s esthetic and functional needs. Additionally, a 3D virtual treatment plan was created with the assistance of 3DDX (Figure 4). The patient desired having fixed restorations supported by dental implants in both maxillary and mandibular arches. All risks, benefits, and alternatives of various treatment options were reviewed with the patient, including dentures, overdentures, and fixed restorations. His treatment plan of choice would consist of fixed hybrid restorations supported by tilted implants in the upper arch to avoid the sinus cavities and axially placed implants in the lower arch.
The implants utilized in this case were OCO Biomedical Engage™ dental implants. These implants are known for their unchallenged high implant stability at placement, which is a critical success factor in these immediate load cases. With the combination of their patented Bull Nose Auger™ tip and mini Cortic-O Thread™, the Engage™ implant system offers practitioners a bone level implant with high initial stability for selective loading options.
The Engage™ implant is self-tapping for an enhanced mechanical lock in the bone. The Bull Nose Auger™ tip will not proceed any deeper than the initial pilot drill preparation locking into the base of the osteotomy. Engage™ implants have a proprietary surface treatment designed to increase the surface area of the implant for optimal bone in-growth and stability. Other dental implant systems in the market with high initial stability may include but are not limited to Hahn (Glidewell Direct), Nobel-Active (Nobel Biocare®), Seven (MIS®), I5 (AB™ Dental USA), Conus 12 (Blue Sky Bio), and AnyRidge® (Megagen).
When performing this many procedures in one visit, I will utilize IV sedation to make the procedure more efficient and comfortable for the patient as well as for myself. Since the patient is sedated, a mouth prop, Logibloc® (Common Sense Dental Products), is used to keep the mouth open. Logibloc’s unique design stabilizes and comfortably supports the jaw while allowing unrestricted visual and physical access to the working area for the provider.
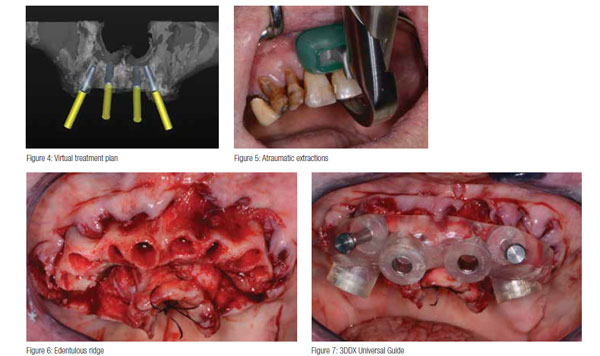 Once the patient was completely sedated and anesthetized, the teeth were extracted in a systematic manner working in sections at a time starting from the anterior maxillary teeth. Acting like a modified Class I lever, the Physics Forceps® (Golden Dental Solutions) were used to atraumatically extract the teeth with the goal of trying not to disturb the underlying bone. The beak of the forceps was placed on the lingual cervical portion of each tooth, where the soft bumper portion was placed on the buccal alveolar ridge at the approximate location of the muco-gingival junction. During the extraction process, the beak grasps the tooth, and the bumper acts as the fulcrum. Extractions were accomplished with only slight wrist action in a buccal direction taking about 40-60 seconds each, depending on the tooth morphology and density of bone (Figure 5).
Once the patient was completely sedated and anesthetized, the teeth were extracted in a systematic manner working in sections at a time starting from the anterior maxillary teeth. Acting like a modified Class I lever, the Physics Forceps® (Golden Dental Solutions) were used to atraumatically extract the teeth with the goal of trying not to disturb the underlying bone. The beak of the forceps was placed on the lingual cervical portion of each tooth, where the soft bumper portion was placed on the buccal alveolar ridge at the approximate location of the muco-gingival junction. During the extraction process, the beak grasps the tooth, and the bumper acts as the fulcrum. Extractions were accomplished with only slight wrist action in a buccal direction taking about 40-60 seconds each, depending on the tooth morphology and density of bone (Figure 5).
Once the teeth were extracted, the tissue was reflected (Figure 6) in order to get the surgical guides seated and fixed with their respectful retention pins. Using these universal surgical guides (Figure 7) provided by 3D Diagnostix, the sites for the implants were begun with a designated 1.8 mm pilot drill from the OCO Biomedical Guided Kit utilizing the Mont Blanc surgical handpiece and Aseptico surgical motor at a speed of 1,200 rpm with copious amounts of sterile saline. Sequential osteotomy formers from the OCO Biomedical Guided Kit were then used to shape the final osteotomies (Figure 8). Once the osteotomies were complete, an implant driver was used to place the dental implants until increased torque was necessary (Figure 9). The ratchet wrench was then connected to the adapter and the implants torqued to final depths reaching a torque level of about 40-50 Ncm.
In the upper arch, four 4.0 mm x 14 mm Engage (OCO Biomedical) dental implants were placed in the areas of teeth Nos. 4, 7, 10, and 13 (Figure 10) to support an All-on-4® restoration. The most distal implants were angled in order to avoid the maxillary sinus cavities and any augmentation in that area. In the lower arch, several different widths and lengths of the Engage (OCO Biomedical) dental implants were placed axially in the remaining ridge.
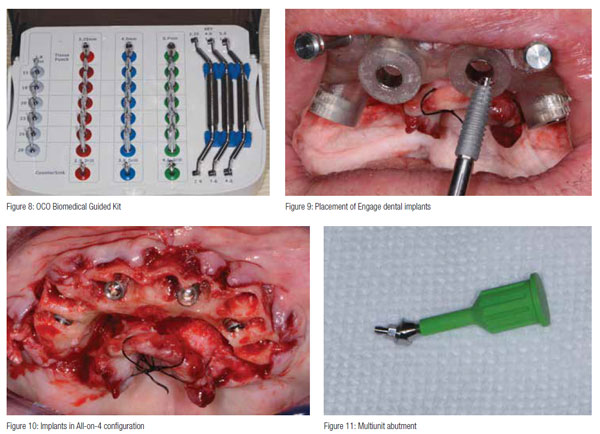 A baseline ISQ reading was taken of these implants utilizing the Osstell ISQ unit. Since the initial readings were all above 65, and the quality of bone after leveling was good, the multiunit abutments (OCO Biomedical) were tightened into the Engage (OCO Biomedical) dental implants for immediate provisionalization (Figure 11).
A baseline ISQ reading was taken of these implants utilizing the Osstell ISQ unit. Since the initial readings were all above 65, and the quality of bone after leveling was good, the multiunit abutments (OCO Biomedical) were tightened into the Engage (OCO Biomedical) dental implants for immediate provisionalization (Figure 11).
Any residual areas around the implants or in the sockets were grafted with a cortical mineralized and demineralized bone grafting material (OCO Biomedical) to optimize the area for regeneration (Figure 12). Primary closure was achieved by suturing the tissue with resorbable sutures.
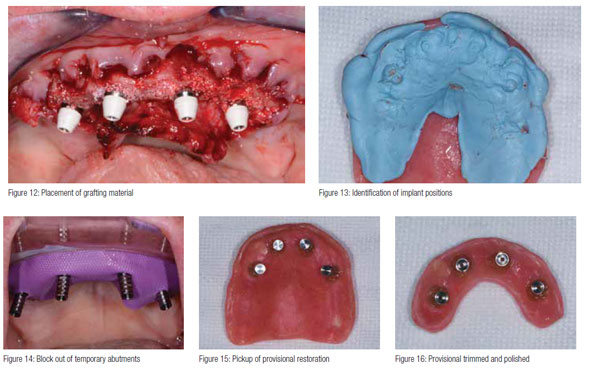 Using Blu-Mousse® (Parkell) bite registration material, the positions of the dental implants was transferred to the record base of the immediate denture (Figure 13) and relieved with a No. 8 round bur (Komet). The immediate provisional restoration was tried in to ensure a passive fit over the temporary abutments. Once confirmed, rubber dam material was placed to avoid the restoration from locking on (Figure 14) and chairside hard reline material (Rebase II, Tokuyama®) placed within recesses around the temporary abutments to pick up the restoration. After the material completely set, the immediate provisional restoration was removed (Figure 15), and any access material trimmed and polished (Figure 16) with the Torque Plus (Aseptico) lab handpiece and acrylic bur (Komet). A similar series of steps was utilized for the mandibular arch and then the bite articulated.
Using Blu-Mousse® (Parkell) bite registration material, the positions of the dental implants was transferred to the record base of the immediate denture (Figure 13) and relieved with a No. 8 round bur (Komet). The immediate provisional restoration was tried in to ensure a passive fit over the temporary abutments. Once confirmed, rubber dam material was placed to avoid the restoration from locking on (Figure 14) and chairside hard reline material (Rebase II, Tokuyama®) placed within recesses around the temporary abutments to pick up the restoration. After the material completely set, the immediate provisional restoration was removed (Figure 15), and any access material trimmed and polished (Figure 16) with the Torque Plus (Aseptico) lab handpiece and acrylic bur (Komet). A similar series of steps was utilized for the mandibular arch and then the bite articulated.
Once the patient awakened from the procedure, a panorex was taken with the CS 8100 3D (Carestream Dental) to confirm the placement and position of the dental implants with their corresponding multiunit abutments and temporary cylinders. The patient could not believe that we were able to extract, level, graft, and place dental implants with corresponding fixed provisional restorations within his surgical appointment (Figure 17).
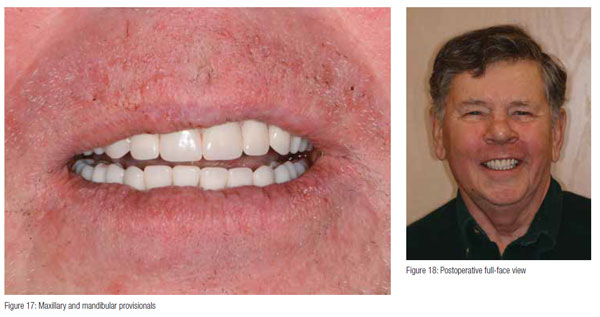 The patient returned 7 days postoperatively with very little discomfort, swelling, or bruising. He was very pleased with his fixed provisional restorations (Figure 18). Now that the patient was no longer anesthetized, the occlusion was checked again to confirm there were no interferences in lateral and protrusive movements. The next step in his treatment would consist of impressions for the definitive upper and lower restorations approximately 4-5 months postoperatively.
The patient returned 7 days postoperatively with very little discomfort, swelling, or bruising. He was very pleased with his fixed provisional restorations (Figure 18). Now that the patient was no longer anesthetized, the occlusion was checked again to confirm there were no interferences in lateral and protrusive movements. The next step in his treatment would consist of impressions for the definitive upper and lower restorations approximately 4-5 months postoperatively.
Conclusion
Having the ability to take a patient from start to finish in a fewer amount of appointments within your practice allows you to position yourself as a provider that can fulfill your patient’s surgical and restorative needs. With the proper training and appropriate materials, a dental provider may provide extraction, grafting, and implant placement within one appointment at one location. Not only does this type of service allow you to reduce the amount of visits for the patient, but also helps maintain the cost to the patient since he/she is not seeing multiple dental providers. Most importantly, this enables the dental provider full control of the surgical and prosthetic outcome. Depending on the patient’s desires, the clinical conditions of the oral environment present, and the skills of the provider, a dentist may choose to extract teeth, level bone, and graft with guided dental implant placement within his/her dental practice.
 Ara Nazarian, DDS, DICOI, maintains a private practice in Troy, Michigan, with an emphasis on comprehensive and restorative care. He is a Diplomate in the International Congress of Oral Implantologists (ICOI). His articles have been published in many of today’s popular dental publications. Dr. Nazarian is the director of the Reconstructive Dentistry Institute. He has conducted lectures and hands-on workshops on esthetic materials and dental implants throughout the United States, Europe, New Zealand, and Australia. He can be reached at 248-457-0500 or online at www.aranazariandds.com.
Ara Nazarian, DDS, DICOI, maintains a private practice in Troy, Michigan, with an emphasis on comprehensive and restorative care. He is a Diplomate in the International Congress of Oral Implantologists (ICOI). His articles have been published in many of today’s popular dental publications. Dr. Nazarian is the director of the Reconstructive Dentistry Institute. He has conducted lectures and hands-on workshops on esthetic materials and dental implants throughout the United States, Europe, New Zealand, and Australia. He can be reached at 248-457-0500 or online at www.aranazariandds.com.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
